
An official website of the United States government
An official website of the United States government
The .gov means it's official.
Federal government websites often end in .gov or .mil. Before sharing sensitive information,
make sure you're on a federal government site.
The site is secure.
The
https:// ensures that you are connecting to the official website and that any
information you provide is encrypted and transmitted securely.
 |
 |
 |
 |
||||
| Front Page | Label | Page 2 | Page 3 | ||||
|
|
|||||||
 |
 |
 |
 |
||||
| Page 4 | Page 5 | Page 6 - 7 | Page 8 | ||||
The front page of the survey will display a mailing label, the Office of Management and Budget statement regarding the length of time it will take to complete the survey, as well as the BLS confidentiality pledge.
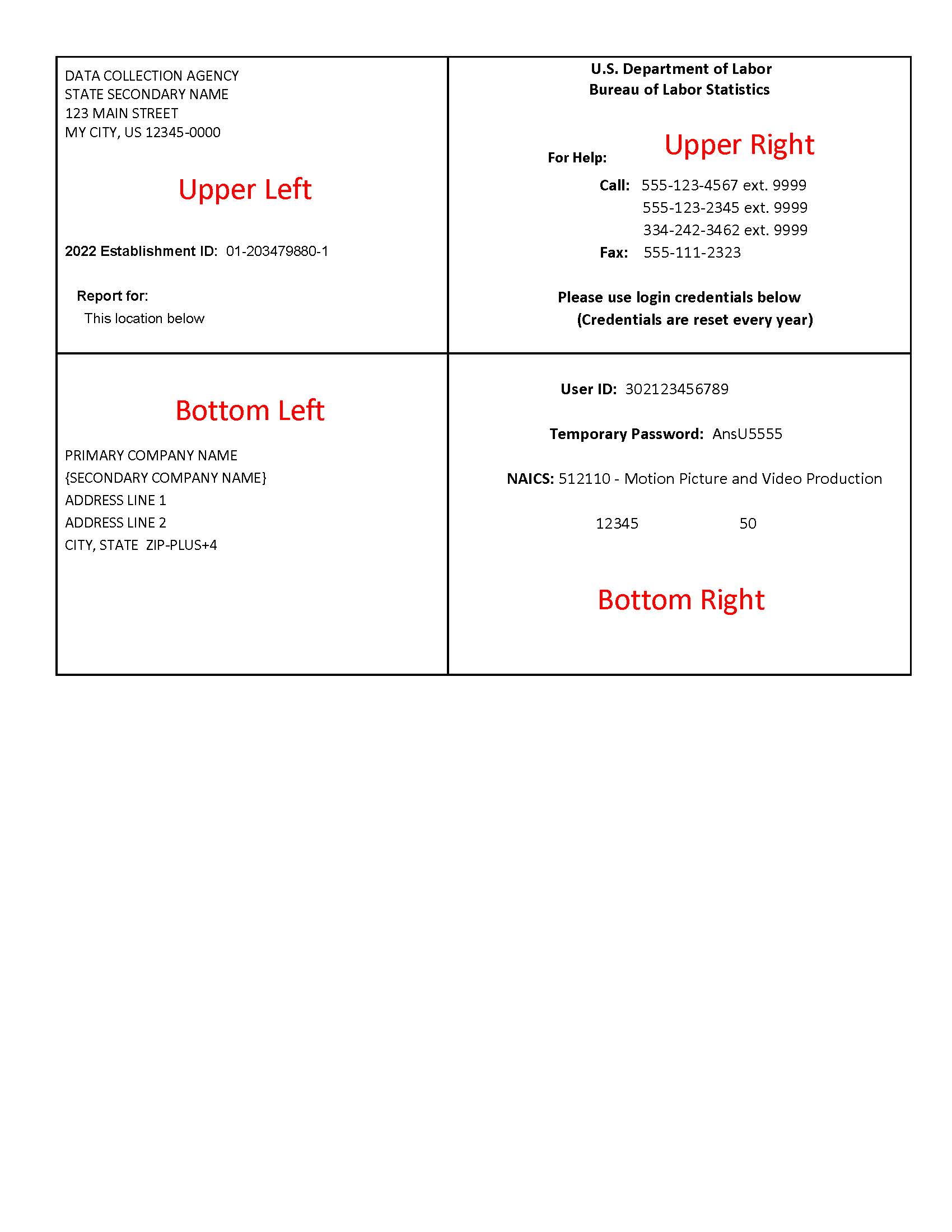
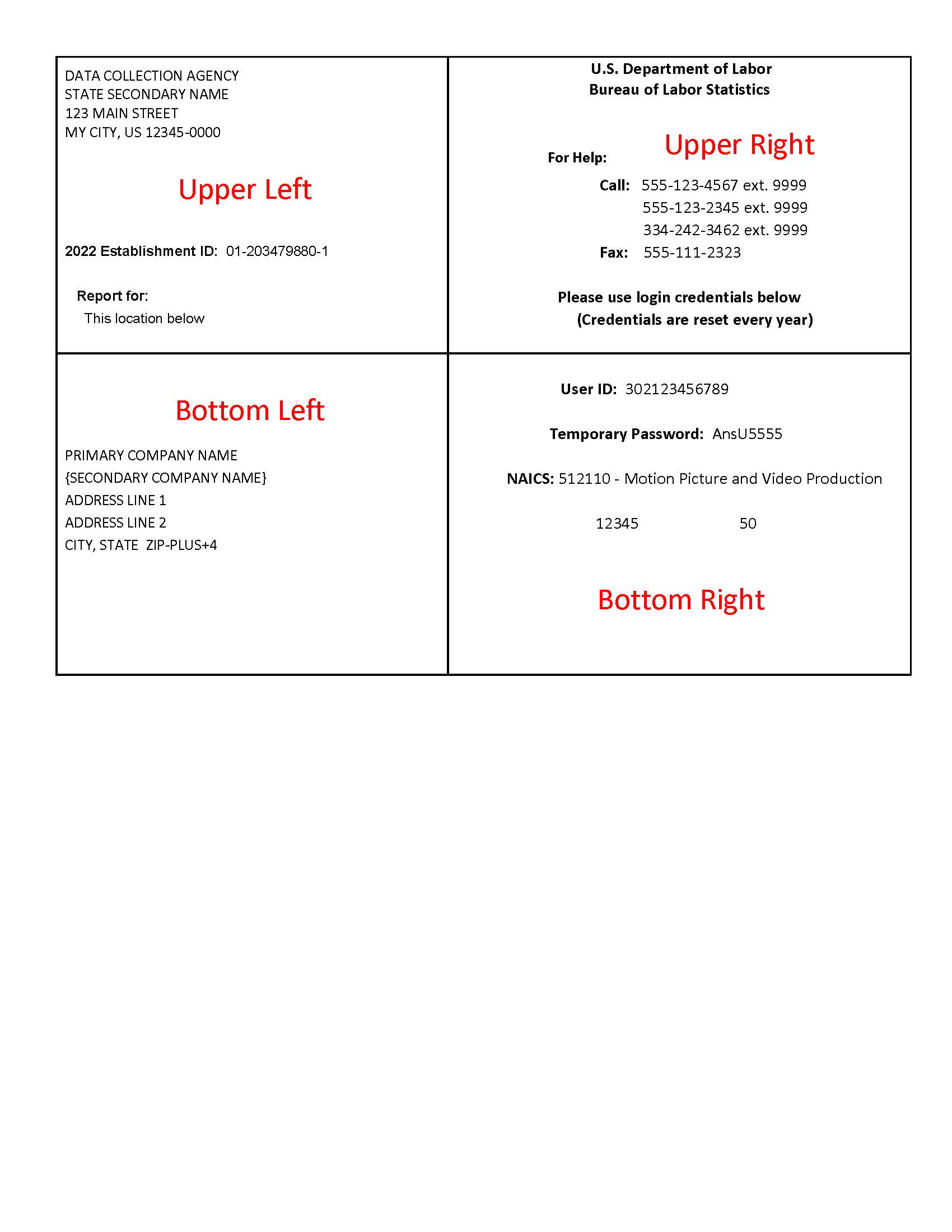
The address of the State or federal agency that is collecting your survey is presented in the upper left of the label. (This address appears through the left hand window of the outgoing mail envelope when the survey is sent to you.) This section also includes Your establishment ID (needed for on-line collection or e-mail collection of your data) and the location(s) for which the survey should be completed. (Listed under 'Report for:')
In the Upper Right of the label are phone and fax numbers you can use for assistance.
Your user ID and temporary password for on-line completion of the survey are located in the Bottom Right section, along with your NAICS Industry code. The remaining items in this portion of the label are for survey use only.
Your company address is presented in the bottom left of the label. If you need to make changes to your company address, you can note those changes on the front of the survey.
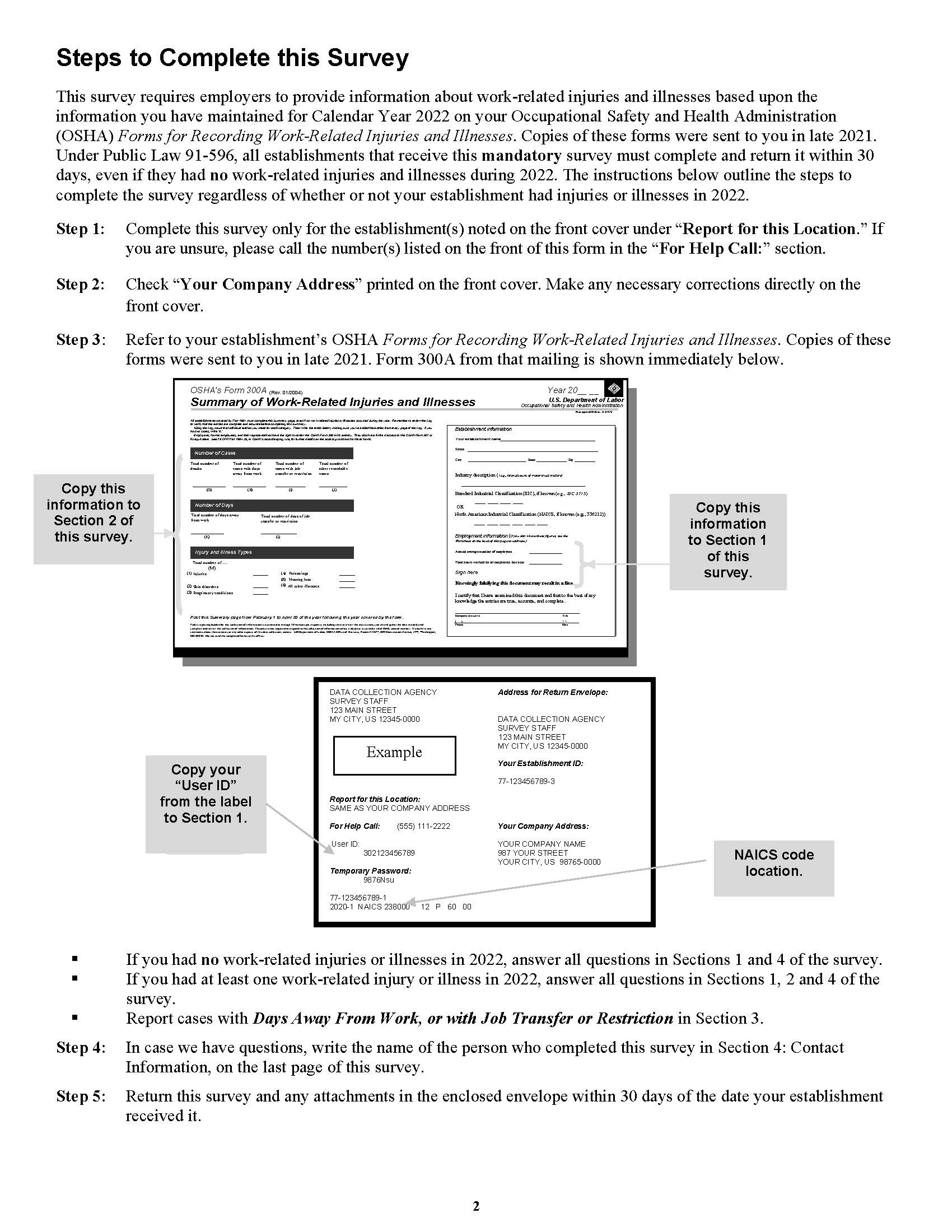
This page presents the steps you need to take to complete the survey.
| Step 1: | Complete this survey only for the establishment(s) noted on the front cover under "Report for: ." If you are unsure, please call the number(s) listed on the front of this form in the "For Help:" section. |
| Step 2: | Check "Your Company Name" printed on the front cover. Make any necessary corrections directly on the front cover. |
| Step 3: | Refer to your establishment's OSHA Forms for Recording Work-Related Injuries and Illnesses. Copies of these forms were mailed to you in late 2022.
|
| Step 4: | In case we have questions, write the name of the person who completed this survey in Section 4: Contact Information, on the last page of this survey. |
| Step 5: | Return this survey and any attachments in the enclosed envelope within 30 days of the date your establishment received it. |
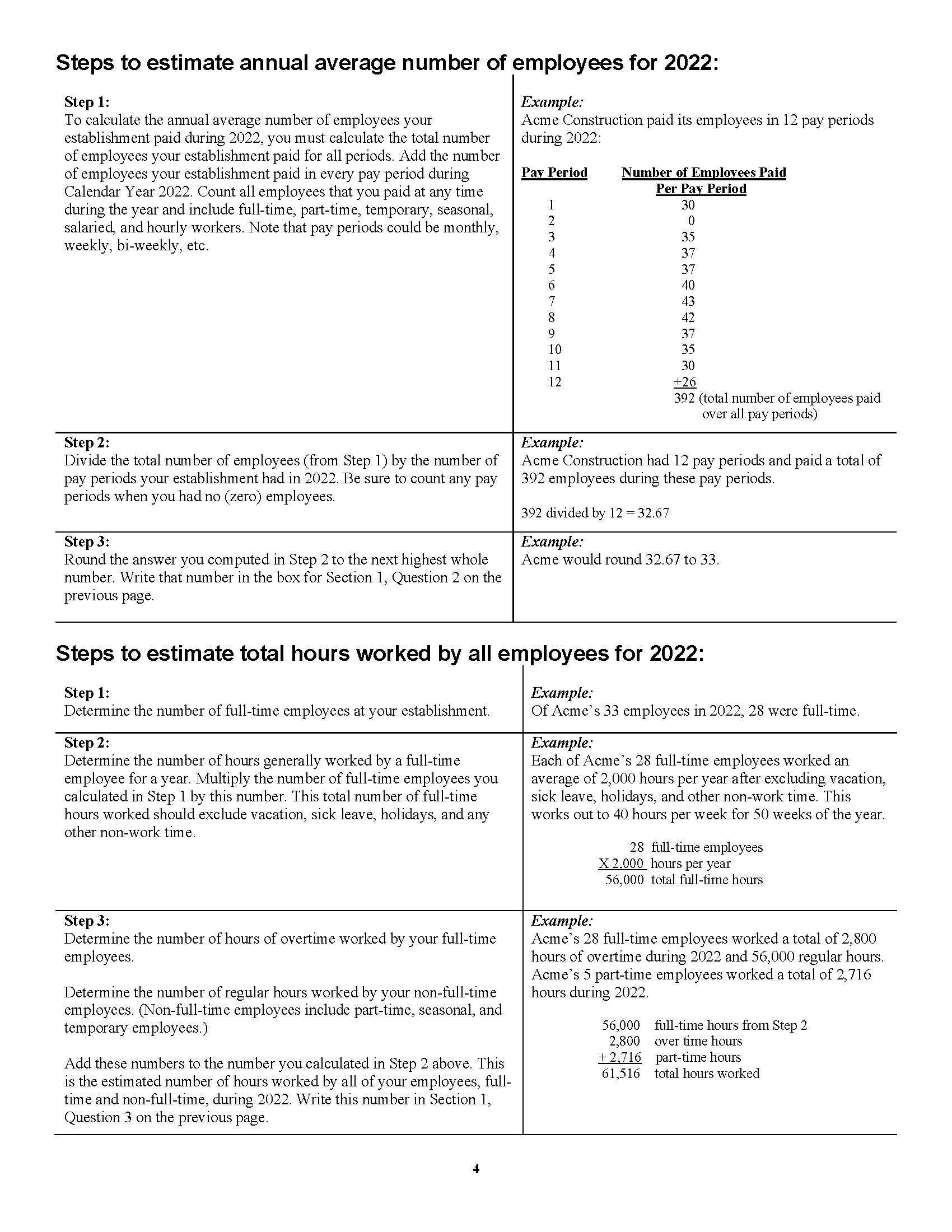
Steps to calculate your annual average number of employees for 2023 and to estimate your total hours worked for 2023 are presented on page 4.
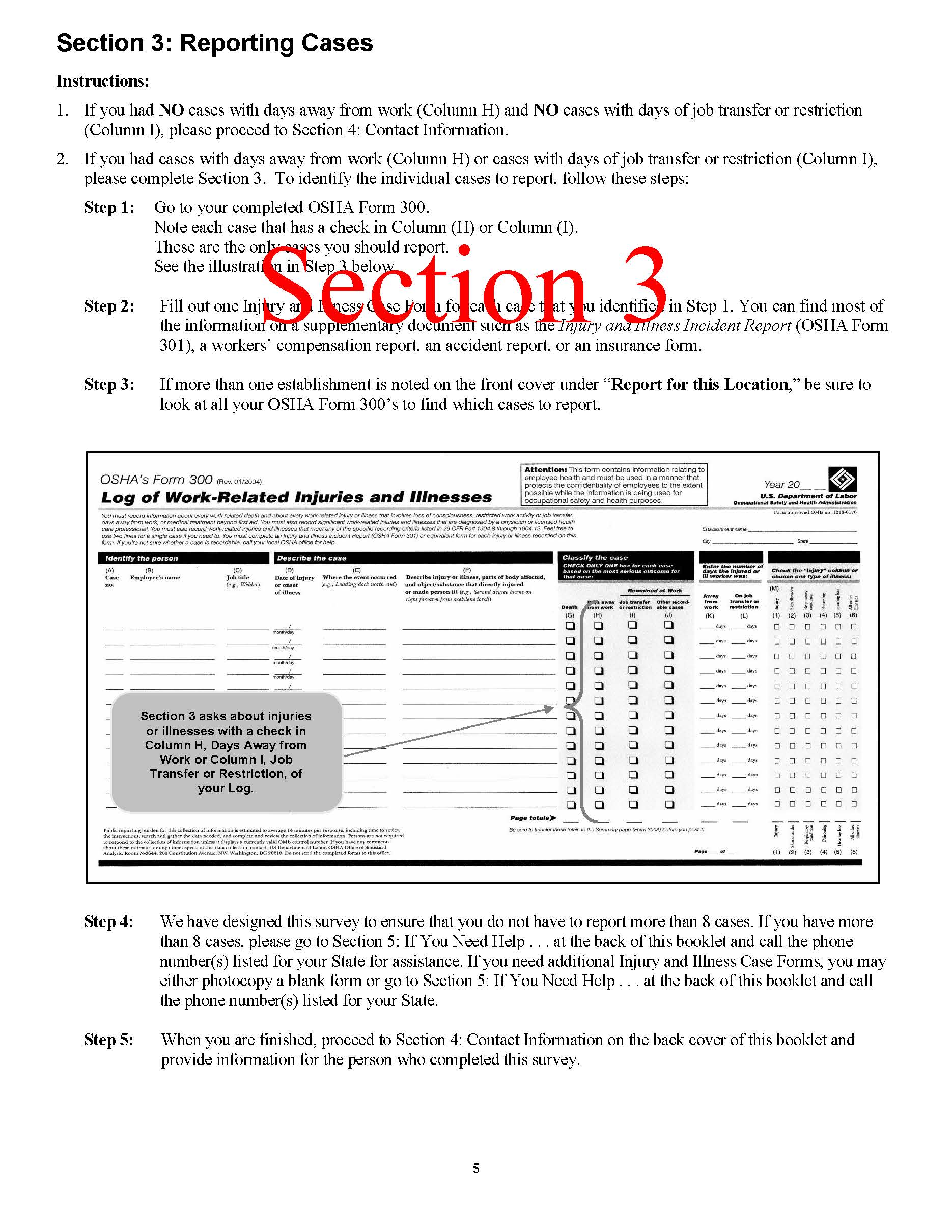
| Step 1: | Go to your completed OSHA Form 300. Note each case that has a check in Column (H) or Column (I). These are the only cases you should report. |
| Step 2: | Fill out one Injury and Illness Case Form for each case that you identified in Step 1. You can find most of the information on a supplementary document such as the Injury and Illness Incident Report (OSHA Form 301), a workers' compensation report, an accident report, or an insurance form. |
| Step 3: | If more than one establishment is noted on the front cover under "Report for this Location," be sure to look at all your OSHA Form 300's to find which cases to report. |
| Step 4: | We have designed this survey to ensure that you do not have to report more than 8 cases. If you have more than 8 cases, please go to Section 5: If You Need Help . . . at the back of this booklet and call the phone number(s) listed for your State for assistance. If you need additional Injury and Illness Case Forms, you may either photocopy a blank form or go to Section 5: If You Need Help . . . at the back of this booklet and call the phone number(s) listed for your State. |
| Step 5: | When you are finished, proceed to Section 4: Contact Information on the back cover of this booklet and provide information for the person who completed this survey. |
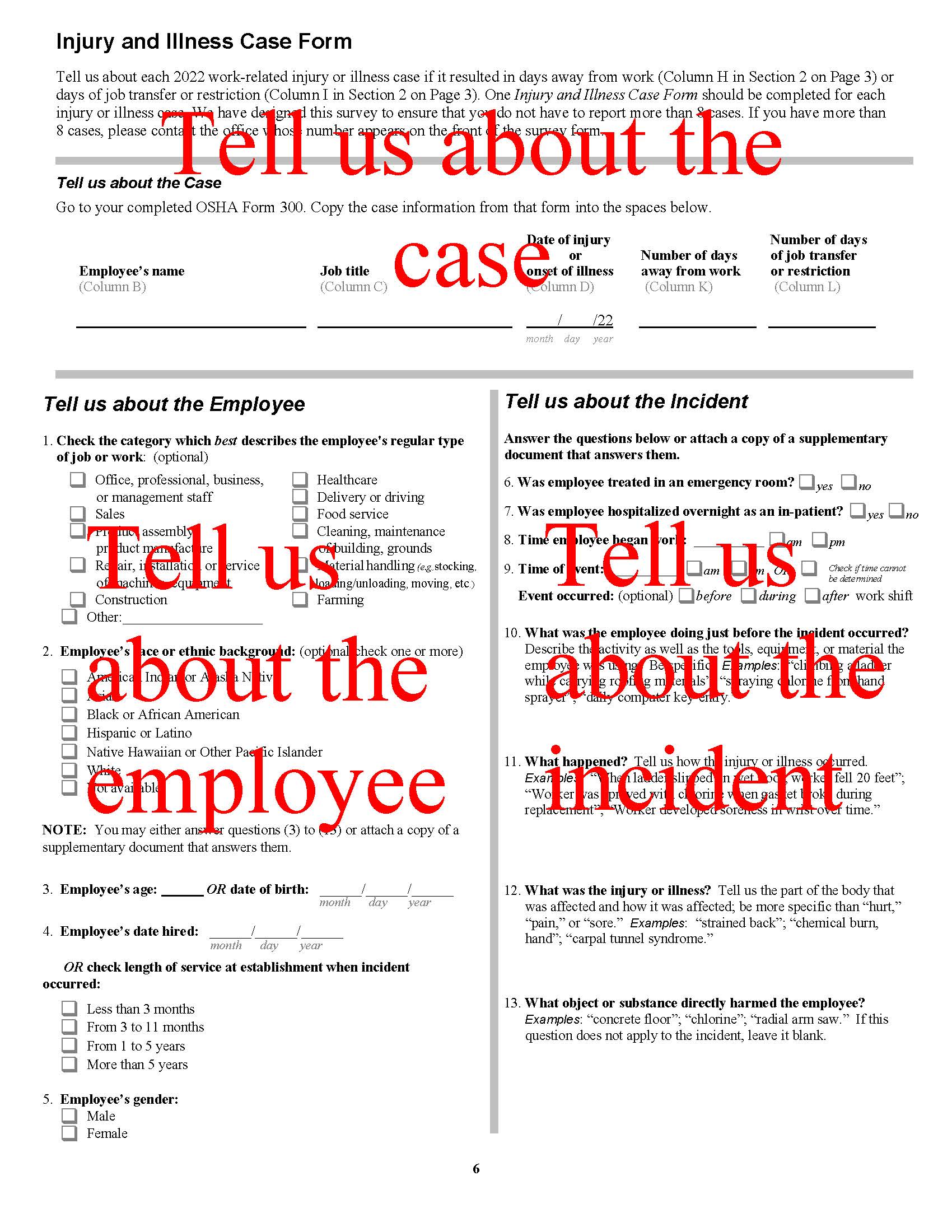
Tell us about the incident - enter the employee's name, job title, date of injury or onset of illness, number of days away from work and number of days of job transfer or restriction.
Tell us about the employee - check the category which best describes the employee's regular type of job (this is optional), check the employee's race or ethnic background (this is optional), enter employee's age at the time of injury or illness OR the employee's date of birth, enter the length of time the employee has worked at this establishment OR check the employee's length of service and finally, check the employee's sex.
Tell us about the incident - check whether the employee was treated in an emergency room and whether the employee was hospitalized overnight as an in-patient. Enter the time the employee began work on the date of the injury, enter the time the injury occurred or check if the time cannot be determined, check if the injury occurred before, during or after the workshift (this is optional). Describe what the employee was doing just before the incident occurred. Describe how the injury or illness occurred. Describe the part of body affected by the injury and how it was affected and finally, describe the object or substance that directly harmed the employee.
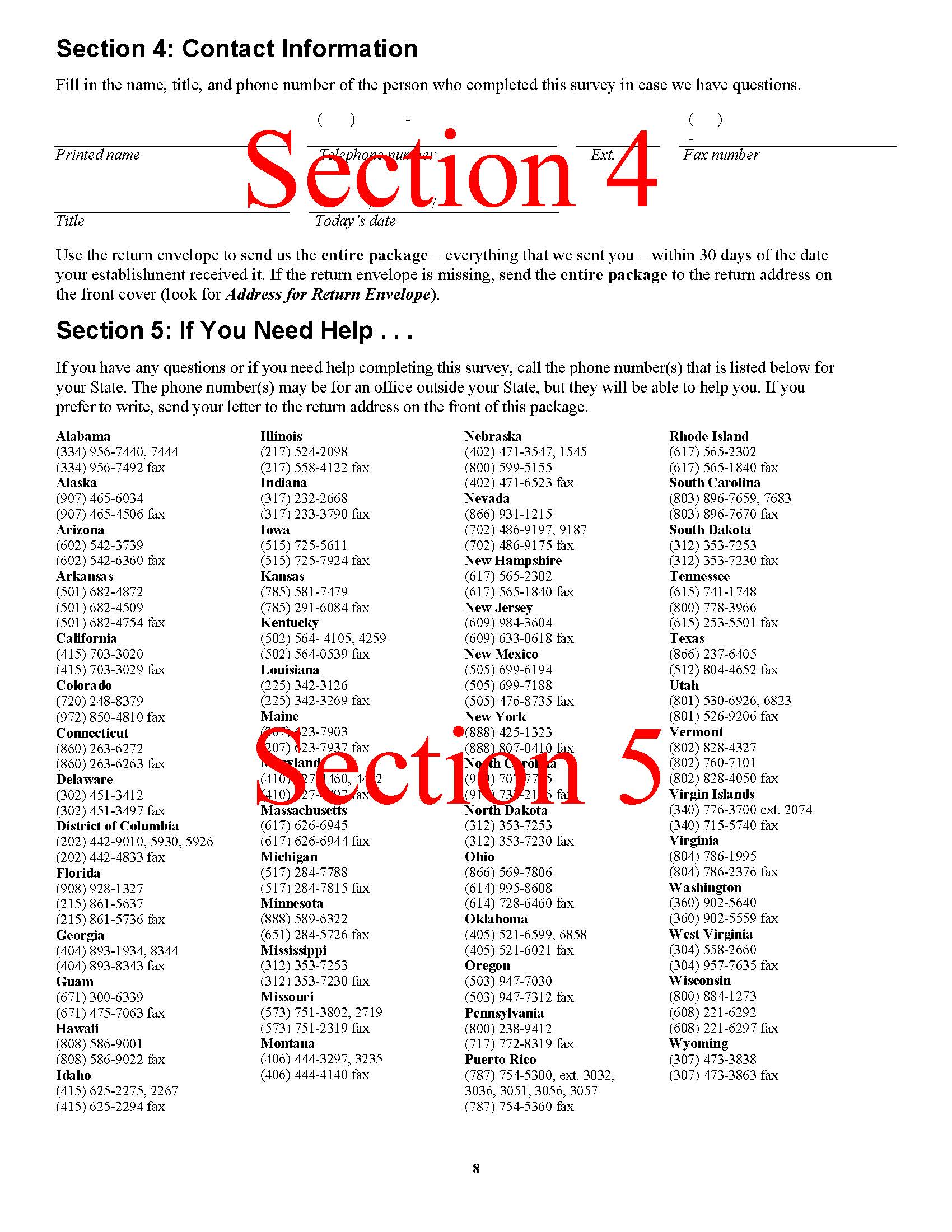
Please let us know who completed the survey in case we need to call with questions.
Contact phone numbers and fax numbers are provided for all of the States collecting this survey.
Last Modified Date: July 21, 2025